Semaglutide: Published Research
A program-by-program bibliographic reference to the semaglutide clinical literature, tracing how the SUSTAIN, PIONEER, STEP, and SELECT trials were designed and what their primary endpoints reported, each attributed to its primary peer-reviewed publication.
For research use only. Not for human consumption. This article is educational reference material. It is not medical advice and is not a recommendation to use any substance.
Introduction
Semaglutide is a long-acting glucagon-like peptide-1 (GLP-1) receptor agonist that has been examined across an unusually large and multi-phase clinical-research record. Rather than a single indication studied in isolation, the published literature is organized into named trial programs, each with its own enrolled population, primary endpoint, and comparator design: the SUSTAIN series (subcutaneous formulation), the PIONEER series (oral co-formulation), the STEP series (body-weight endpoints), and the SELECT cardiovascular-outcome trial in participants without diabetes. This article summarizes the design logic and primary reported findings of representative trials in each program, with every outcome attributed to its primary peer-reviewed publication. No aggregate efficacy judgment or comparative ranking is offered by Sparta Labs; the receptor pharmacology underlying these programs is treated separately in the semaglutide mechanism-of-action reference.
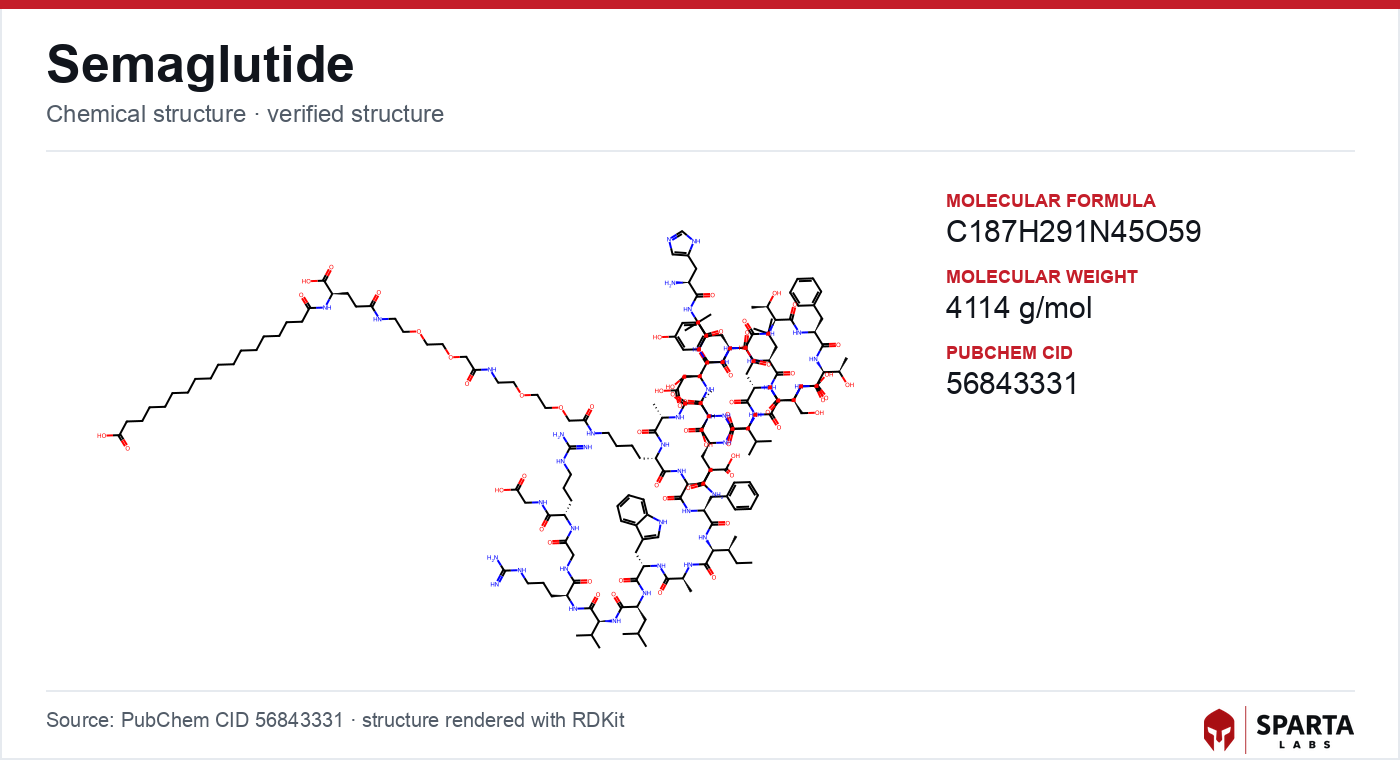
Figure: chemical structure of semaglutide.
How the Trial Programs Were Designed
A recurring feature of the semaglutide literature is that trial architecture was dictated by regulatory context as much as by scientific question. Following 2008 U.S. Food and Drug Administration guidance requiring new type 2 diabetes therapies to rule out excess cardiovascular risk, cardiovascular-outcome trials (CVOTs) became a structural requirement rather than an optional add-on [1]. This is why the earliest large semaglutide trials, SUSTAIN-6 and PIONEER 6, were built as event-driven, non-inferiority CVOTs against a composite major adverse cardiovascular event (MACE) endpoint, adjudicated by blinded independent committees, rather than as conventional glycemic-efficacy studies.
The programs diverge in their primary endpoints. Glycated hemoglobin (HbA1c) change from baseline anchored most SUSTAIN and PIONEER glycemic trials; percentage change in body weight and the proportion of participants reaching a five-percent reduction threshold were co-primary endpoints in the STEP obesity program; and time to first MACE event was primary in the CVOTs. These distinctions matter when reading the literature, because outcomes are not directly interchangeable across programs even when the same molecule is studied.
SUSTAIN-6: The Subcutaneous Cardiovascular Signal
SUSTAIN-6 was a randomized, double-blind, placebo-controlled trial at 230 sites across 20 countries, enrolling 3,297 adults with type 2 diabetes at high cardiovascular risk, with standard of care continued in both arms. Marso and colleagues reported the primary MACE composite (cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke) in the New England Journal of Medicine in 2016 [2]. The event occurred in 6.6% of the semaglutide group versus 8.9% of the placebo group (hazard ratio 0.74; 95% CI, 0.58 to 0.95), meeting the pre-specified non-inferiority threshold and reaching nominal superiority [2].
Findings from research models do not establish safety or efficacy in humans. Sparta Labs makes no claims about the use of this compound.
A distinctive and closely examined observation from SUSTAIN-6 was a numerically higher rate of retinopathy complications in the semaglutide arm, which the authors flagged as warranting further study and which shaped ophthalmologic monitoring in later work [2]. This detail is frequently cited as an example of how a CVOT can surface a signal outside its primary endpoint that then redirects subsequent research design.
PIONEER 6 and the Oral Formulation Problem
Peptides are ordinarily poorly absorbed when taken by mouth, so the oral semaglutide studied in the PIONEER program was co-formulated with the permeation enhancer SNAC (sodium N-[8-(2-hydroxybenzoyl)amino]caprylate) to enable gastric absorption, a formulation strategy that made oral delivery of a GLP-1 peptide analytically and clinically distinct from the injectable form. PIONEER 6 was an event-driven, randomized, double-blind, placebo-controlled CVOT in 3,183 patients with type 2 diabetes at high cardiovascular risk. Husain and colleagues published the results in the New England Journal of Medicine in 2019 [3].
The hazard ratio for the primary MACE composite was 0.79 (95% CI, 0.57 to 1.11), meeting the pre-specified non-inferiority margin [3]. All-cause mortality was numerically lower in the oral semaglutide group (hazard ratio 0.51; 95% CI, 0.31 to 0.84), which the authors explicitly framed as hypothesis-generating because the trial was not powered to test individual mortality components [3]. PIONEER 6 established the cardiovascular-safety basis that supported regulatory authorization of the first orally administered GLP-1 receptor agonist. Comparisons with dual and triple incretin agonists in the same broader pharmacological class are summarized in the tirzepatide published-research summary and the mazdutide research overview.
The STEP Program: Body-Weight Endpoints Without Diabetes
The STEP series shifted the primary endpoint from glycemia to body weight and, importantly, enrolled participants without diabetes, making it the program most often discussed in the obesity literature.
STEP 1: 68-Week Primary Result
STEP 1 randomized 1,961 adults with a body mass index of 30 kg/m² or above (or 27 kg/m² or above with at least one weight-related comorbidity) and without diabetes to 68 weeks of once-weekly subcutaneous semaglutide or placebo alongside lifestyle intervention. Wilding and colleagues reported a mean body-weight change from baseline of −14.9% with semaglutide versus −2.4% with placebo, and 86.6% of the semaglutide group reached the five-percent-reduction threshold versus 47.6% with placebo [4]. Gastrointestinal adverse events, predominantly nausea and diarrhea, were reported in 82.8% of the semaglutide group versus 63.2% of placebo, characterized by the authors as consistent with the known profile of the GLP-1 receptor agonist class [4].
STEP 5: Durability at Two Years
STEP 5 was designed to test whether outcomes persisted over 104 weeks. Garvey and colleagues, publishing in Nature Medicine in 2022, enrolled 304 adults without diabetes who had overweight or obesity with at least one comorbidity and reported a mean body-weight change of −15.2% with semaglutide versus −2.6% with placebo at week 104, with 77.1% of the semaglutide group reaching the five-percent threshold [5]. The authors noted these two-year outcomes were consistent with earlier time points in the program [5].
SELECT: Extending the Evidence Base to a Non-Diabetic Cardiovascular Population
SELECT (Semaglutide Effects on Cardiovascular Outcomes in People with Overweight or Obesity) was a multicenter, double-blind, randomized, placebo-controlled, event-driven superiority CVOT at 804 sites across 41 countries. Lincoff and colleagues published results in the New England Journal of Medicine in 2023 [6]. The trial enrolled 17,604 participants with established cardiovascular disease and overweight or obesity but without diabetes, a population not represented in the SUSTAIN-6 or PIONEER 6 CVOTs.
At a mean follow-up of 39.8 months, the primary MACE composite occurred in 6.5% of the semaglutide group versus 8.0% of placebo (hazard ratio 0.80; 95% CI, 0.72 to 0.90; P<0.001 for superiority) [6]. Because body weight and multiple cardiometabolic risk factors changed simultaneously in the semaglutide arm, the mechanistic basis for the observed risk reduction in this non-diabetic population is described by the authors as unresolved and an active area of investigation, rather than attributable to any single pathway [6].
Emerging and Ongoing Research Directions
Beyond the flagship programs, semaglutide has been examined in metabolic liver disease. Newsome and colleagues reported a phase 2, randomized, double-blind, placebo-controlled trial in biopsy-confirmed non-alcoholic steatohepatitis (NASH) in the New England Journal of Medicine in 2021, a study frequently cited as the design precedent for the larger phase 3 hepatology program that followed [7]. Reading these hepatology results alongside the metabolic-endpoint programs illustrates how a single GLP-1 receptor agonist has been evaluated against histological, glycemic, weight, and cardiovascular endpoints in separate, independently powered trials.
Investigators engaged in GLP-1 receptor pharmacology can obtain third-party-verified reference material through semaglutide from Sparta Labs. Sourcing, identity, and purity-verification considerations relevant to analytical work are discussed in the semaglutide sourcing and verification reference.
References
-
U.S. Food and Drug Administration. Guidance for Industry: Diabetes Mellitus — Evaluating Cardiovascular Risk in New Antidiabetic Therapies to Treat Type 2 Diabetes. December 2008. Available at: fda.gov/media/71297/download
-
Marso SP, Bain SC, Consoli A, et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2016;375(19):1834–1844. doi:10.1056/NEJMoa1607141. PubMed PMID: 27633186. Link
-
Husain M, Birkenfeld AL, Donsmark M, et al. Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2019;381(9):841–851. doi:10.1056/NEJMoa1901118. PubMed PMID: 31185157. Link
-
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989–1002. doi:10.1056/NEJMoa2032183. PubMed PMID: 33567185. Link
-
Garvey WT, Batterham RL, Bhatta M, et al. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nat Med. 2022;28(10):2083–2091. doi:10.1038/s41591-022-02026-4. PubMed PMID: 36216945. Link
-
Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389(24):2221–2232. doi:10.1056/NEJMoa2307563. PubMed PMID: 37952131. Link
-
Newsome PN, Buchholtz K, Cusi K, et al. A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis. N Engl J Med. 2021;384(12):1113–1124. doi:10.1056/NEJMoa2028395. PubMed PMID: 33185364. Link
Disclaimer. Statements in this article have not been evaluated by the Food and Drug Administration. This compound is not intended to diagnose, treat, cure, or prevent any disease. Sparta Labs sells research-use-only materials. Content is provided for educational and informational purposes only and does not constitute medical advice. Consult a qualified medical professional for any health concerns.
Frequently asked questions
Why were semaglutide's earliest large trials designed as cardiovascular-outcome trials?
After 2008 U.S. Food and Drug Administration guidance required new type 2 diabetes therapies to rule out excess cardiovascular risk, cardiovascular-outcome trials became a structural requirement. SUSTAIN-6 and PIONEER 6 were consequently built as event-driven, non-inferiority studies against a composite major adverse cardiovascular event endpoint rather than as conventional glycemic-efficacy trials.
What did the SUSTAIN-6 trial report?
Marso and colleagues reported in the New England Journal of Medicine in 2016 that the primary major adverse cardiovascular event composite occurred in 6.6% of the semaglutide group versus 8.9% of placebo among 3,297 adults with type 2 diabetes at high cardiovascular risk (hazard ratio 0.74; 95% CI, 0.58 to 0.95). The authors also flagged a numerically higher rate of retinopathy complications in the semaglutide arm as warranting further study.
How does oral semaglutide differ from the injectable form in the research literature?
The oral form studied in the PIONEER program was co-formulated with the permeation enhancer SNAC to enable gastric absorption of the peptide. PIONEER 6, published by Husain and colleagues in 2019, was the cardiovascular-outcome trial that established the safety basis supporting authorization of the first orally administered GLP-1 receptor agonist.
What population did the SELECT trial study that earlier trials did not?
SELECT, reported by Lincoff and colleagues in the New England Journal of Medicine in 2023, enrolled 17,604 participants with established cardiovascular disease and overweight or obesity but without diabetes. This population was not represented in the earlier SUSTAIN-6 or PIONEER 6 cardiovascular-outcome trials, extending the evidence base to a non-diabetic group.
Has semaglutide been studied in metabolic liver disease?
Newsome and colleagues reported a phase 2, randomized, double-blind, placebo-controlled trial in biopsy-confirmed non-alcoholic steatohepatitis in the New England Journal of Medicine in 2021. That study is frequently cited as the design precedent for the larger phase 3 hepatology program that followed.