PT-141 (Bremelanotide): Mechanism of Action
A mechanism-focused reference on bremelanotide (PT-141): its origin as a Melanotan-II metabolite, the alpha-MSH message sequence, MC3R/MC4R agonism, and hypothalamic Gs/cAMP signaling. Educational reference.
For research use only. Not for human consumption. This article is educational reference material. It is not medical advice and is not a recommendation to use any substance.
From Melanotan-II to a Melanocortin Message Peptide
PT-141, later designated bremelanotide, did not begin as a stand-alone drug candidate. It emerged from work on the synthetic tanning agent Melanotan-II, when investigators observed that the parent compound was subject to metabolic cleavage and that one of its degradation products retained melanocortin receptor activity while lacking the C-terminal amide that drives pigmentary signaling [1]. Bremelanotide is that fragment stabilized as a discrete cyclic heptapeptide (Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-Lys]-OH). Its structural relationship to Melanotan-II is examined in the Melanotan-2 mechanism of action article; the two share the lactam-bridged core that defines this chemical series.
The peptide's design centers on the conserved "message sequence" His-Phe-Arg-Trp that all endogenous melanocortins carry as the minimal motif required for receptor engagement [1]. Substituting the native L-phenylalanine with D-phenylalanine and constraining the backbone through an Asp-Lys lactam bridge produced a molecule with enzymatic resistance and altered receptor selectivity relative to the linear alpha-melanocyte-stimulating hormone (alpha-MSH) template. This article surveys the receptor pharmacology, hypothalamic circuitry, and secondary physiological signals that the peer-reviewed literature attributes to that structure. A broader chemistry summary is available in the PT-141 research overview.
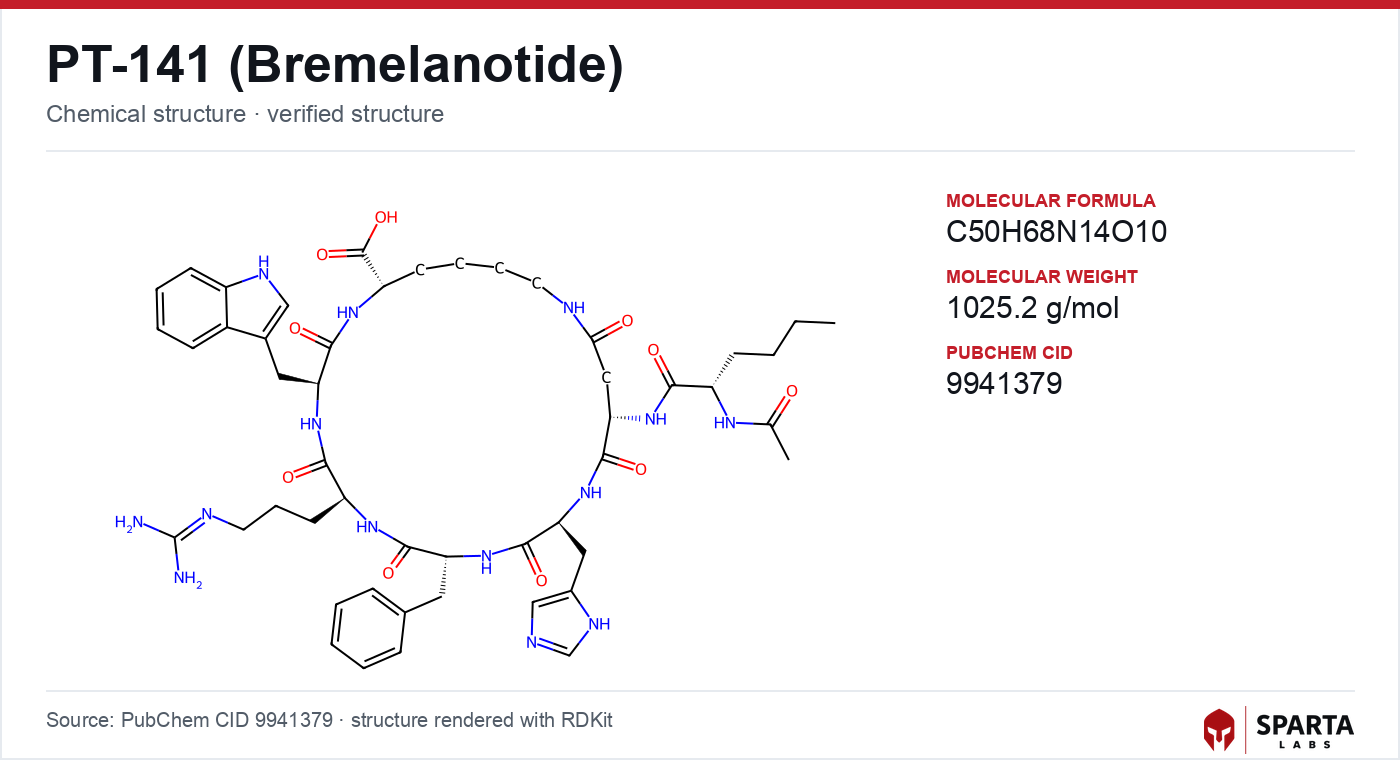
Figure: chemical structure of PT-141.
The Melanocortin Receptor Family and Bremelanotide's Selectivity
The melanocortin system comprises five class A G protein-coupled receptors (MC1R through MC5R) that respond to peptides cleaved from proopiomelanocortin (POMC), including adrenocorticotropic hormone (ACTH) and the alpha-, beta-, and gamma-MSH peptides [1]. The subtypes segregate by tissue: MC1R governs melanocyte pigmentation, MC2R is the dedicated ACTH receptor of the adrenal cortex, MC5R is expressed in exocrine glands, and MC3R and MC4R are the two subtypes concentrated in the central nervous system.
Bremelanotide behaves as a non-selective agonist across several melanocortin receptors but with functional emphasis on the two central subtypes. Molinoff and colleagues (2003), reviewing the preclinical characterization of PT-141, described the compound as an MC3R/MC4R-preferring agonist whose central activity distinguished it from vasoactive agents acting on peripheral smooth muscle [1]. The reduced pigmentary signaling relative to Melanotan-II reflects the loss of the parent molecule's terminal amide, which the melanocyte-expressed MC1R depends on for full activation.
Findings from research models do not establish safety or efficacy in humans. Sparta Labs makes no claims about the use of this compound.
Because bremelanotide engages MC4R, it sits within the same receptor pharmacology that governs energy balance and neuroendocrine signaling. The distribution and function of that receptor were mapped through genetic and anatomical studies discussed in the following sections.
MC4R as a Hypothalamic Signaling Node
The physiological importance of MC4R was established through targeted gene disruption. Huszar and colleagues (1997) reported that mice lacking a functional melanocortin-4 receptor developed hyperphagia, increased body mass, and disrupted energy homeostasis, identifying MC4R as a non-redundant node in the hypothalamic circuits that integrate metabolic and neuroendocrine signals [2]. This work placed MC4R at the center of a signaling architecture in which agonist peptides such as alpha-MSH and endogenous antagonists such as agouti-related protein (AgRP) exert opposing tone.
MC4R is expressed at high density in the paraventricular nucleus of the hypothalamus, the arcuate nucleus, the brainstem, and limbic structures including regions of the amygdala [1][2]. This anatomical map is central to interpreting bremelanotide's pharmacology: an agonist that reaches these receptors acts within circuits already characterized for their role in integrating internal state and motivated behavior, rather than at peripheral vascular targets. The endogenous melanocortin tone at these sites, set by the balance of POMC-derived agonists and AgRP-derived antagonism, provides the physiological backdrop against which an exogenous agonist operates.
Intracellular Coupling: Gs, cAMP, and Downstream Transcription
MC3R and MC4R are canonically coupled to the stimulatory G protein Gs. Agonist binding promotes exchange of GDP for GTP on the Galpha-s subunit, which activates adenylyl cyclase and raises intracellular cyclic adenosine monophosphate (cAMP). Elevated cAMP activates protein kinase A (PKA), which in turn can phosphorylate the transcription factor cAMP response element binding protein (CREB), coupling receptor occupancy to changes in neuronal gene expression [1]. This Gs/cAMP/PKA cascade is the shared second-messenger logic across the melanocortin family, with receptor subtype and cell context determining the physiological readout.
The literature also documents that melanocortin receptors display biased and pleiotropic coupling beyond the canonical Gs pathway in some cellular contexts, a nuance that complicates simple structure-to-signal predictions [1]. For bremelanotide specifically, the reported downstream consequence of central MC3R/MC4R engagement is neuronal activation within the hypothalamic and limbic circuits noted above, rather than a peripheral vasodilatory response.
Central Circuit Engagement in Preclinical Models
The neural correlates of melanocortin agonism have been probed in rodent models of motivated behavior. Studies from the melanocortin behavioral pharmacology literature reported that central administration of melanocortin agonists, including bremelanotide, was associated with activation of hypothalamic circuits as indexed by immediate-early gene expression, and with changes in centrally organized behaviors in animal models [3]. These preclinical observations were foundational to the interpretation of bremelanotide as a centrally acting compound rather than a peripheral agent.
This circuit-level framing carried through the compound's clinical development. The randomized phase 3 program summarized in the PT-141 published research article reported changes across validated psychometric endpoints in premenopausal participants, and the pharmacological rationale for those trials rested on the central MC4R mechanism characterized in the preclinical work rather than on any peripheral vascular action [4]. The interpretive gap between rodent circuit activation and human clinical endpoints remains a defining feature of the mechanistic literature.
Cardiovascular Signal as a Melanocortin Effect
A recurring secondary observation in the bremelanotide literature is a transient elevation in blood pressure following administration, characterized in the FDA-reviewed clinical program that supported the compound's approval [4]. This signal is consistent with the broader melanocortin pharmacology, because central melanocortin tone contributes to sympathetic outflow and cardiovascular regulation. Rather than an off-target artifact, the blood-pressure effect is interpreted in the literature as an on-mechanism consequence of melanocortin receptor engagement, and it informed formulation and administration decisions during clinical development [4]. The distinction between the intended central pharmacology and this cardiovascular signal illustrates why melanocortin agonists are characterized across multiple physiological axes rather than a single endpoint.
Limits of Current Mechanistic Understanding
Several features of bremelanotide's mechanism remain incompletely resolved in the published literature. The relative contribution of MC3R versus MC4R agonism to its measured effects has not been fully dissected, in part because subtype-selective pharmacological tools that cleanly separate the two receptors in vivo are limited [1]. The precise neural pathways linking central MC4R occupancy to the human clinical endpoints reported in the phase 3 program are characterized at the level of hypothesis rather than settled circuit anatomy [4].
The melanocortin system's inherent complexity compounds this uncertainty: overlapping agonist and antagonist tone, distributed receptor expression across hypothalamic, limbic, and cortical structures, and context-dependent intracellular coupling all resist reduction to a single pathway [1]. The alpha-MSH-derived tripeptide KPV, which engages overlapping melanocortin signaling with a different functional profile, is examined in the KPV mechanism of action article and illustrates how fragments of the same parent hormone can diverge pharmacologically. Batch-level Certificate of Analysis documentation for research applications is available on the PT-141 product page.
References
-
Molinoff PB, Shadiack AM, Earle D, Diamond LE, Quon CY. PT-141: a melanocortin agonist for the treatment of sexual dysfunction. Ann N Y Acad Sci. 2003;994:96-102. PMID: 12851303. DOI: 10.1111/j.1749-6632.2003.tb03167.x. Available at: https://pubmed.ncbi.nlm.nih.gov/12851303/
-
Huszar D, Lynch CA, Fairchild-Huntress V, Dunmore JH, Fang Q, Berkemeier LR, et al. Targeted disruption of the melanocortin-4 receptor results in obesity in mice. Cell. 1997;88(1):131-141. PMID: 9019399. DOI: 10.1016/s0092-8674(00)81865-6. Available at: https://pubmed.ncbi.nlm.nih.gov/9019399/
-
Pfaus JG, Shadiack A, Van Soest T, Tse M, Molinoff P. Selective facilitation of sexual solicitation in the female rat by a melanocortin receptor agonist. Proc Natl Acad Sci U S A. 2004;101(27):10201-10204. PMID: 15226504. DOI: 10.1073/pnas.0400491101. Available at: https://pubmed.ncbi.nlm.nih.gov/15226504/
-
Simon JA, Kingsberg SA, Portman D, Williams LA, Krop J, Jordan R, et al. Bremelanotide for the treatment of hypoactive sexual desire disorder: two randomized phase 3 trials. Obstet Gynecol. 2019;134(5):899-908. PMID: 31599840. DOI: 10.1097/AOG.0000000000003500. Available at: https://pubmed.ncbi.nlm.nih.gov/31599840/
Disclaimer. Statements in this article have not been evaluated by the Food and Drug Administration. This compound is not intended to diagnose, treat, cure, or prevent any disease. Sparta Labs sells research-use-only materials. Content is provided for educational and informational purposes only and does not constitute medical advice. Consult a qualified medical professional for any health concerns.
Frequently asked questions
What is the origin of PT-141 (bremelanotide)?
Bremelanotide was identified as an active metabolite of the synthetic melanocortin agonist Melanotan-II. Investigators observed that a cyclic fragment retained melanocortin receptor activity after loss of the parent compound's C-terminal amide, and this fragment was developed as the discrete heptapeptide bremelanotide. Molinoff and colleagues (2003) reviewed its preclinical characterization as an MC3R/MC4R-preferring agonist.
Which melanocortin receptors does bremelanotide act on?
The published literature characterizes bremelanotide as a non-selective melanocortin agonist with functional emphasis on the two central subtypes, MC3R and MC4R. These are the melanocortin receptors concentrated in the central nervous system, in contrast to MC1R (pigmentation), MC2R (the ACTH receptor), and MC5R (exocrine glands).
Why is MC4R central to bremelanotide's reported mechanism?
MC4R is expressed at high density in hypothalamic and limbic structures. Huszar and colleagues (1997) reported that mice lacking a functional MC4R developed hyperphagia and altered energy homeostasis, identifying the receptor as a non-redundant hypothalamic signaling node. Bremelanotide's activity at MC4R places it within these characterized central circuits.
What intracellular pathway do MC3R and MC4R use?
Both receptors are canonically coupled to the stimulatory G protein Gs. Agonist binding activates adenylyl cyclase and raises intracellular cyclic AMP, which activates protein kinase A and can lead to phosphorylation of the transcription factor CREB. This Gs/cAMP/PKA cascade is the shared second-messenger logic across the melanocortin receptor family.
Why is a blood-pressure signal discussed alongside bremelanotide's mechanism?
A transient blood-pressure elevation was characterized in the FDA-reviewed phase 3 clinical program. Because central melanocortin tone contributes to sympathetic and cardiovascular regulation, the literature interprets this as an on-mechanism consequence of melanocortin receptor engagement rather than an off-target artifact.